

1 Introduction
Research Impact (RI) is a broad topic of scientometrics to support the progress of science and monitoring the influence of efforts made by the government, institutions, societies, programs, and individual researchers. There are several documented and popular RI assessment methods developed by individuals and organisations for evaluating the research of a particular programme or general-purpose. This intent has created the diversity in evaluation methods, frameworks and scope. Some approaches focus only on the impacts related to academic recognition and use, such as Bibliometric Measures. However, the growing technology, educational networking, effective and targeted research strategies, and regular monitoring of RI are reducing the gap between the research producers and consumers. As a result, the horizon of RI is expanding and covering other areas of impacts such as on economy, society, and environment.
Many individuals and organizations have introduced measures and indicators for assessing the RI. Nevertheless, due to diversity in nature and scale of RI, not a single method is considered robust and complete (Vinkler, 2010). Therefore, new measures and indicators are being introduced on time to time basis according to the interest and availability of resources of the method designers (Canadian Academy of Health Sciences, 2009). Additionally, higher availability of national and international funding for health sciences is critically influencing the science of RI assessment (Heller & de Melo-Martín, 2009). It means there are more indicators, measures, and frameworks for health-related research than any other areas of science. Resultantly, there is a considerable gap available for generalizability and transformability of health-related efforts to rest of the science.
At large, this study aims to discover the evidence-based diversity of RI indicators and to develop a method. In this regard, Nomenclature of RI indicators is developed based on divide and rule principle to achieve the objective. Additionally, taxonomical analysis is presented based on the primary components of nomenclature. This effort is a step forward to develop a robust and inclusive RI assessment method. The concept of this paper was initially presented in the 17th International Conference on Scientometrics and Informetrics (ISSI 2019) in the form of a poster (Arsalan, Mubin, & Al Mahmud, 2019).
2 Review of literature
As per the broader understanding, metrics and indicators are different. It is clear from the semantics as “indicator” indicates the research impact, whereas metrics are the measurement of research impact. According to P. Vinkler (2010), an indicator should be read as a meaningful representative, which indicate the performance of a system as per its design objective. Metrics, on the other side, provide additional quantitative information about the impact of a system (Lewison, 2003). However, diversity of effects can create a problematic situation to measure all aspects quantitatively. Therefore, pragmatically indicators have the potential to illustrate useful and broader impacts as compared to the metrics (Vinkler, 2010).
There are multiple reasons for diversity in research impact indicators. For instance, Bennett et al. (2016) explained 10-points criteria for making research impact indicators from a technical and contextual point of view. In this regard, indicators should be specific, validated, reliable, comparable, substantial, accessible, acceptable, appropriate, useable, and feasible. Consequently, diversity in criteria required range of indicators to fulfil the conditions in diversified context. Canadian Academy of Health Sciences (2009) explained another reason for this diversity, i.e. strategy of indicator selection. This strategy describes three basic principles.
The indicator should answer the specific question of evaluation
The indicator should satisfy the level of aggregation
The indicator should be read with other indicators to complement the strength of evaluation
In other words, every indicator only explains the impact of research in minimal dimension, covers a very specific level of aggregation, and has a very limited power of defining the research impact (REF, 2012). As a result, we need a bundle of indicators that fulfil the strategic requirements of evaluators.
“Nomenclature” is a combination of two Latin words viz. “nomen” means “name” and “calare” means “to call”. It is a scientific process in any discipline to assign the names to essential components according to the predefined rules and standards (Hayat, 2014). Generally, these rules are outlined in the form of a classification scheme. Therefore, for nomenclature, the classification system is highly significant. Longabaugh et al. (1983) introduced the problem-focused nomenclature in medical science, which is a coding system with a specific objective. They argued that the problem-focused approach provides better control for organizing and problem management. The similar concept can be applied in any branch of science to organize the objects concerning a problem-focused classification system.
Classification and organization of research impact indicators are not new (Vinkler, 2010). However, the nomenclature or taxonomy approach is missing. Therefore, standardization is globally missing. Every effort of research impact assessment distinctly organized the indicators according to the technical and contextual requirements. Nonetheless, based on the context, the classification scheme of indicators can be arranged in four groups.
Impact Categories and Domains
Impact Time and Pathways
Impact in Specific Dimension
Uncategorised
In many research impact assessment methods, the adopted organization of impact indicators is based on impact categories and domains. These methods are wide-scope and open to select indicators in any of their classes (Bernstein et al., 2006). Payback framework for assessing the impact of health research is one of the classical methods falls under this group, for instance (Buxton & Hanney, 1996). It was developed by the Health Economics Research Group at Brunel University in 1996 by Buxton and Hanney (1996). It organizes the indicators in multi-dimensional categories including knowledge, research benefits, political, and administrative benefits, health sector benefits, and broader economic benefits.
The second group that follows the impact time and pathways are based on the concept of output and outcome. The understanding of the difference between output and outcome was first explained by United Way of America (1996) in the form of logic modelling. This model explicitly defines inputs, process and outputs in the form of resources, activities and products, respectively. Whereas, the outcome is a benefit to the population of interest. Weiss (2007) split the outcomes of health research into initial, intermediate, and long-term impacts. This time-bound approach represents a sequence or a chain of effects. For instance, awareness of new research in decision-making community is an initial outcome. That awareness can lead to a change in clinical practice as an intermediate outcome. Ultimately, the long-term outcome is the improvement in the health of patients.
The third approach is exclusive. Many organizations and individual researchers are keen to know the impact of research only in one area in depth. One example is the monetary value approach presented by Deloitte Access Economics (2011). In this approach, all indicators and measures are solely related to the economic impacts of research. Some other methods are organization-specific where a scoring system is limited in scope and developed in a local context. We cannot fit them in any above mentioned organized structure, for instance, The Wellcome Trust’s Assessment Framework (Wellcome Trust, 2009), Matrix Scoring System (Wiegers et al., 2015), and Royal Netherlands Academy of Arts and Sciences Approach (VSNU, KNAW, & NWO, 2009).
Although the organizations of indicators within a research impact framework has been a mandatory part of every evaluation method, there is still a need to organize the indicators based on criteria and rules. A classic example of diversity and heterogeneity can be seen in REF (2012) where more than 100 indicators are applied based on subject domains and target areas of socio-economic interest. There is still a need to adopt a mechanism where these indicators can be generalized and transformed on taxonomical structures.
3 Method
We systematically explored the literature databases, including Scopus, WebMD, ACM DL, IEEE Xplore, Web of Science and Google Scholar to collect research articles providing RI assessment indicators and methods. In many cases, organizations published the frameworks and guidelines in the form of technical reports; therefore, grey literature was also considered.
Multiple combinations of literature-searching keywords were used with their synonyms. These include but not limited to the “research impact,” “research productivity,” “research quality,” “research impact indicators,” “research impact assessment,” “research impact assessment method,” “research impact assessment framework,” “scientometric indicators,” “bibliometric indicators,” “economic indicators,” “social indicators,” and “environmental indicators.” The purpose of using a combination of these keywords was to identify theoretical or applied studies related to the research impact assessment. In theoretical or conceptual studies, we found the constructs and mechanisms of research impact assessment methods applied studies provided the demonstration of assessment methods in the form of case studies. We also found some review articles, which provided a comparison of different RI assessment approaches. However, in this study, we mainly focused on the preparation of RI indicators. Due to using multiple combinations of keywords and databases, we found the significant repetition of the same studies, which we removed with the help of EndNote software. In this study, we extracted indicators from conceptual studies. We used NVivo 12 software for annotation and coding. For deciphering the nomenclature, indicators were disintegrated based on their lexical and conceptual structures as discussed in the Results section. For improving the result of coding, inter-coder reliability was applied on 10% of data and conflicts were resolved with the help of discussion.
The base of the cognitive structure of defined nomenclature in this study is the “every indicator is a contextual-function to explain the impact”. The primary constructs of an indicator are function and context. Function refers to the “correspondence”, “dependence relation”, “rule”, “operation”, “formula” or “representation” as defined by Vinner and Dreyfus (1989). It explains the relationship between the two domains “research” and “impact”. In other words, impact (y) is a function of research (x), i.e. y=f(x). At large, in scientometrics understanding, the functional operation can be “improvement”, “recognition”, “reduction”, “replacement” etc. (see Table 1 for examples). The indicator is a subjective measure of a system-dependent phenomenon which is always described in its contextual understanding by a system designer (Vinkler, 2010). Therefore, the indicator’s function is always applied in a specific context. For instance, “improvement in patient care system”, in this indicator, the patient care system represents the context of the healthcare system, and it is critically important for researchers, funders, institutes and support organisations related to the health sciences (Trochim et al., 2011).
Structure of Indicator (I) = F + C
Where, F = Function, and C = Context
Whereas
C = t + d
Where, t = target area, and d = impact domain
Table 1 Nomenclature of Indicator with Examples. |
| Functions (F) |
|---|
| Improvement / Addition / Reduction This function of indicator explains the addition or enhancement of an existing phenomenon in quantitative or qualitative form. (Example: Improvement in economic gains such as increased employment, health cost cut (Weiss, 2007)) |
| Creation This function of indicator focuses on the creativity in the form of the development of new knowledge, theory, technique, method, technology, approach, opportunity or any workflow. (Example: Creation of prevention methods for clinical practice (Trochim et al., 2011)) |
| Recognition This function explains the recognition of effort in the form of outstanding quality by the peers or experts such as in the form of awards, promotions, meritorious selection and work showcasing etc. This recognition can be of the research, the researcher or the research institute. (Example: Receiving an award on research (Kuruvilla et al., 2006)) |
| Obsoleting / Replacing This function elaborates the policy, law, regulation to obsolete or disuse the existing phenomena to overcome the future negative impacts. (Example: Change in law to obsolete the existing method of drug approval (Maliha, 2018)) |
| Context (C) |
| Target (t) Contextual targets in research impact science include knowledge, service, policy, law, guideline, system, technology, procedure, method, framework, workflow, publication, patent, product, stakeholder, citation, literature gaps, intellectual challenges, scholarly issues, relationships, collaborations, and networks etc. These are the key areas but usually partial in contextual understanding. |
| Domain (d) The contextual domain is the main area or field of interest of the indicator system designer such as health, education, economy, environment, academia, medical science, chemistry, history, multidisciplinary etc. The main body of knowledge and elaboration of indicators are always from the domain language. The domain is the main component of the indicator, which specialised the context and application of the indicator. However, the level of the domain is subject to the interest and perspective of impact evaluator. |
4 Results and discussion
4.1 Search outcome and identification of indicators
The result of the literature search is more than one thousand studies (1,152), where research impact was published in the form of theoretical papers, case studies and review articles. However, after excluding studies where research impact was assessed in case-studies by using any method developed by elsewhere, only 36 conceptual studies were left. In the conceptual studies, we found out more than 500 research impact indicators. For this study, we selected 119 indicators for preparing the nomenclature (see Appendix 1).
4.2 Nomenclature
In many cases, an indicator is self-explanatory and well written in a proper construct-based structure such as Development of mitigation methods for reducing environmental hazards and losses from natural disasters (Grant et al., 2010). However, similar to an algebraic expression, sometimes constructs are obscured but well understood by the users. For instance, in Number of citations, where, Function and the contextual domain is missing but well recognized as an Increased number of bibliometric citations, where, Function is the addition, the contextual target is citations, and the domain is bibliometrics.
This contextual nomenclature of indicators allows focussing on context and function irrespective of the selection of the words and lexical structure of the indicator. Additionally, it strengthens the idea of contextual generalisability, which is very helpful in extending the applications and scope of the indicators. For example, in use of research in the development of medical technology (where, Function = development/creation, Contextual Target = Technology, and Contextual Domain = Healthcare). This indicator can be generalised on the variable domain such as use of research in the development of technology (where, Function = development/creation, Contextual Target = Technology, and Contextual Domain = variable [generalized]).
4.3 Taxonomical analysis
In analyzed indicators, most of the indicators are functionally related to the improvements in the current state of affairs (63%), mainly focused on future research, services and methods (Figure 1 ). However, recognition of research (23%) in the form of bibliometric, rewards and other citations is also considerably highlighted in the literature-based list of indicators. Creativity and development (14%) are also the prevailing influence of research, which is reflected in indicators mentioning the creation of new knowledge, technique, research teams, drugs etc. More than half (59%) of the indicators attempt to explore the impact in the academic domain (Figure 2 ), e.g. Where and how the research is recognised? What knowledge, methods and collaborations are formed? What challenges, issues and gaps are addressed? Knowledge domains related to the social systems and services are second in coverage (26%) that primarily focus on the healthcare, education and justice systems. Economic policies and services also have a good share (11%) in literature-based indicators. Although, during the last two decades, the impact of research on improving the environment and sustainability has also emerged in various indicators, its representation is quite low.
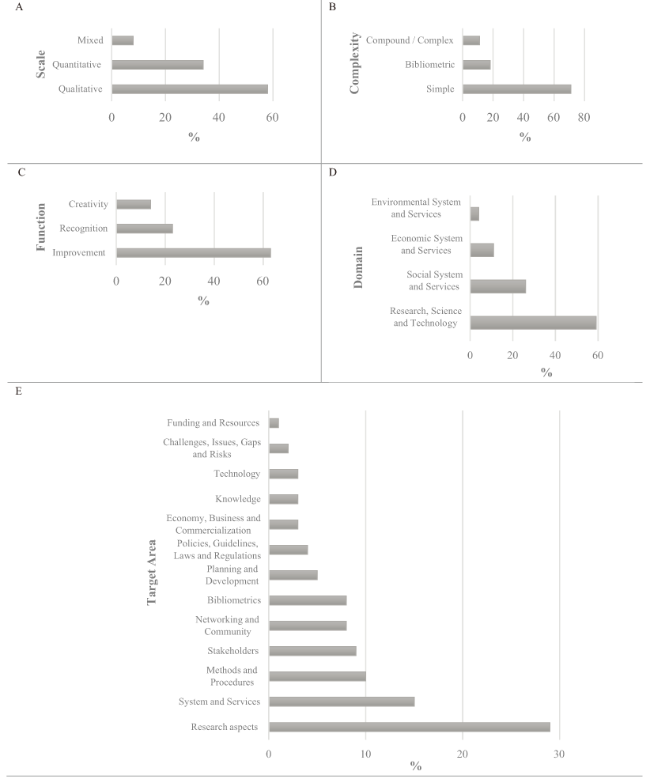
Figure 1. Evidence-based taxonomical characteristics of indicators, (A) Scale of indicators, (B) Complexity of indicators, (C) Functions of indicators, (D) Domains of indicators, and (E) Target areas of indicators. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 2. Cross-constructs distribution of indicators characteristics, (A) Functional distribution of target areas in indicators, (B) Domain distribution of target areas in indicators, and (C) Functional distribution of domains in indicators. |
4.4 Limitations of the study
In this study, 119 indicators were interpreted and coded for nomenclature and taxonomy. However, the inclusion of more indicators may change the results of classification. Another aspect which may affect the outcome of the study is consistency in interpretation and coding of indicators. Although it was improved by using the intercoder reliability method on 10% indicators, rule-based text mining techniques may improve the results.
5 Conclusion and future direction
The study categorized the research impact indicators based on their characteristics and scope. Furthermore, a concept of evidence-based nomenclature of research impact indicator has been introduced to generalize and transform the indicators. For building nomenclature and classification, one hundred and nineteen indicators were selected and coded in NVivo software. The nomenclature was developed based on the principle “every indicator is a contextual-function to explain the impact”. Every indicator was disintegrated in three parts (essential ingredients of nomenclature), i.e. Function, Domain, and Target Areas. It is observed that in literature, the primary functions of research impact indicators are improvement, recognition and creation/development. The focus of research impact indicators in literature is more towards the academic domain, whereas the environment/sustainability domain is least considered. As a result, research impact related to the research aspects is considered the most. Other target areas include system and services, methods and procedures, networking, planning, policy development, economic aspects and commercialisation etc.
The study provided a novel approach in scientometrics for generalizability and transformability of research impact indicators. It explored the diversity of indicators and demonstrated the generalization based on fundamental constructs, i.e. function, domain and target area. As a result, a research impact indicator can be modified and applied to multiple research disciplines.
Author contributions
The first author is a PhD student under the supervision of the second author and co-supervision of the third author. Therefore, Mudassar Arsalan (M.Arsalan@westernsydney.edu.au) contributed to data collection, analysis and drafting of the paper, whereas Omar Mubin (O.Mubin@westernsydney.edu.au) and Abdullah Al Mahmud (aalmahmud@swin.edu.au) facilitated in conceptualization and reviewing the article.
Appendix 1. Indicators identified in literature
| Ref | Indicator | Reference | Measure | Qualitative/Quantitative |
|---|---|---|---|---|
| 1 | Identification of research gaps, questions and new research dimension | (Heller & de Melo-Martín, 2009; Kuruvilla, Mays, Pleasant, & Walt, 2006; W. M. Trochim, Marcus, Masse, Moser, & Weld, 2008; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 2 | Development of a new technique for data collection and new data | (Heller & de Melo-Martín, 2009; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 3 | Creation of a research method or extension of existing by involving new approach and technique | (Kuruvilla et al., 2006; W. M. Trochim et al., 2008) | Yes / NoŦ | Qualitative |
| 4 | Defining the concept and subject vocabulary in a more comprehensive way | (Mankoff, Brander, Ferrone, & Marincola, 2004; W. M. Trochim et al., 2008) | Yes / NoŦ | Qualitative |
| 5 | Formation of research groups and collaborate in multidimensional research | (S. R. Hanney, Grant, Wooding, & Buxton, 2004; Heller & de Melo-Martín, 2009; Kuruvilla et al., 2006; W. M. Trochim et al., 2008) | Yes / NoŦ | Qualitative |
| 6 | Recruitment of skilled researchers | ../../../../Google Drive/Working/001 PhD Work/00103 Paper 1/Drafting/Indicators v2.xlsx - RANGE!_ENREF_68 (Heller & de Melo-Martín, 2009) | How many researchers are recruited? | Quantitative |
| 7 | Development of communities of science, new grant programmes; replication and new research | (S. Hanney, Buxton, Green, Coulson, & Raftery, 2007) | Yes / NoŦŦ | Mixed |
| 8 | Effective planning and addressing future research | ../../../../Google Drive/Working/001 PhD Work/00103 Paper 1/Drafting/Indicators v2.xlsx - RANGE!_ENREF_51 (Gordon & Meadows, 1981) | Yes / NoŦ | Qualitative |
| 9 | Research capacity building for an individual or a group of researchers | (Buxton & Hanney, 1996; Raftery, Hanney, Greenhalgh, Glover, & Blatch-Jones, 2016) | How many researchers are trained? | Quantitative |
| 10 | Preparing a better procedure for researchers induction | (Heller & de Melo-Martín, 2009; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 11 | Improvement in ethical approval processes for better decisions and timeliness | (Pober, Neuhauser, & Pober, 2001; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 12 | Formation of new research teams and projects | (Pober et al., 2001) | How many projects and teams are established? | Quantitative |
| 13 | Successful completion of ongoing research with the achievement of set targets | (Weiss, 2007) | Yes / NoŦŦ | Mixed |
| 14 | Retention of research team by involving in productivity and future research | (Heller & de Melo-Martín, 2009; Kuruvilla et al., 2006; Nathan, 2002) | How many members are retained? | Quantitative |
| 15 | Advancement in numbers and quality of research and research teams | (Nathan, 2002; Pober et al., 2001; W. M. Trochim et al., 2008; Weiss, 2007) | Yes / NoŦŦ | Mixed |
| 16 | Enhancement of research process, behaviour and procedural protocols | (Heller & de Melo-Martín, 2009; Pober et al., 2001; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 17 | Recognition and leadership of researchers in the research domain | (Kuruvilla et al., 2006; Pober et al., 2001) | Yes / NoŦ | Qualitative |
| 18 | Improvement of research communication between researchers and research organizations | (Heller & de Melo-Martín, 2009; Mankoff et al., 2004) | Yes / NoŦ | Qualitative |
| 19 | Serving of research staff on a higher level in more advanced organizations at national and international level | (Kuruvilla et al., 2006; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 20 | Improvement in research culture and overall environment | (Heller & de Melo-Martín, 2009; Kessler & Glasgow, 2011; Mankoff et al., 2004; Pober et al., 2001; Sung et al., 2003) | Yes / NoŦ | Qualitative |
| 21 | Identification and overcoming of the research process constraints | (Heller & de Melo-Martín, 2009; Pober et al., 2001) | Yes / NoŦ | Qualitative |
| 22 | Improved willingness and tangible measures for practice-based and applied research | (Westfall, Mold, & Fagnan, 2007) | Yes / NoŦ | Qualitative |
| 23 | Development of improved analytical methods for existing data | (Kessler & Glasgow, 2011; Kuruvilla et al., 2006; W. M. Trochim et al., 2008; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 24 | Improvement in multi-disciplinary research methods | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 25 | Creation of methods for cross domains results in interpretation and synthesis | (Kuruvilla et al., 2006; Pang et al., 2003) | Yes / NoŦ | Qualitative |
| 26 | Embracing the innovative methods for measuring the research outcome | (Dougherty & Conway, 2008; W. M. Trochim et al., 2008) | Yes / NoŦ | Qualitative |
| 27 | Discovery of new or advanced research findings | (Lavis, Ross, McLeod, & Gildiner, 2003; Mankoff et al., 2004) | Yes / NoŦ | Qualitative |
| 28 | Discovery of novel knowledge or innovative techniques | (S. R. Hanney et al., 2004; Kalucy, Jackson-Bowers, McIntyre, & Reed, 2009; Lavis et al., 2003; W. Trochim, Kane, Graham, & Pincus, 2011) | Yes / NoŦ | Qualitative |
| 29 | Demonstration of an efficient way of treatment | (Lavis et al., 2003; W. Trochim et al., 2011; Woolf, 2008) | Yes / NoŦ | Qualitative |
| 30 | Development of new research devices or products for better results | (ARC, 2018; Kalucy et al., 2009; Lavis et al., 2003; Mankoff et al., 2004; Pang et al., 2003) | Yes / NoŦŦ | Mixed |
| 31 | Obtaining patents for new devices or products | (ARC, 2018; Kuruvilla et al., 2006; Lavis et al., 2003; Lewison, 2003; Sarli, Dubinsky, & Holmes, 2010) | How many patents are obtained? | Quantitative |
| 32 | Identification or validation of new biomarkers for better healthcare | (Lavis et al., 2003; Zerhouni, 2007) | Yes / NoŦ | Qualitative |
| 33 | Use of research outcomes and discoveries into the advancement of research related to animals and humans | (Pober et al., 2001; Woolf, 2008; Zerhouni, 2007) | Yes / NoŦ | Qualitative |
| 34 | Receiving an award on research | (Kuruvilla et al., 2006) | How many awards are received? | Quantitative |
| 35 | The increment in number and proportion of research grant submissions and awards | (ARC, 2018; Lavis et al., 2003; Lewison, 2003; Weiss, 2007) | What is the proportion of success of grant award? | Quantitative |
| 36 | Increase in the quantity of publications in high ranking journals as a research outcome | (Buxton & Hanney, 1996; Kuruvilla et al., 2006; Lewison, 2003; Pang et al., 2003; Weiss, 2007) | How many publications are produced in high ranking journals? ŦŦŦ | Quantitative |
| 37 | Increase in the total impact factor gained by publishing research in high ranking journals | (ARC, 2018; Archambault & Lariviere, 2009; RAND Europe, 2006; Weiss, 2007) | How much impact factor is gained? ŦŦŦ | Quantitative |
| 38 | Increase in the conference papers and presentations organized on national or international levels. | (ARC, 2018; Kalucy et al., 2009; Lewison, 2003) | How many conference papers and presentations are produced? ŦŦŦ | Quantitative |
| 39 | Increase in the number of citations of research outcome | (ARC, 2018; Garfield, 2006; S. R. Hanney et al., 2004; Kuruvilla et al., 2006; RAND Europe, 2006; Weiss, 2007) | How many citations are obtained? ŦŦŦ | Quantitative |
| 40 | Increase in media appearance of researchers or research organizations for their findings and its relation to the public | (Kuruvilla et al., 2006; Lewison, 2003) | How many times appeared in media? | Quantitative |
| 41 | Popularity and acceptance of research-based knowledge and techniques in masses (e.g. change in community-based health practice or education system) | (Kalucy et al., 2009; Kuruvilla et al., 2006; Lewison, 2003; Pang et al., 2003; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 42 | Participation of researchers as a member of the research journal editorial board or become a journal editor | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 43 | Dissemination and reach of research outcome to more audiences | (Kalucy et al., 2009; Kuruvilla et al., 2006; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 44 | IF2-Index | (Boell & Wilson, 2010) | Index Value ŦŦŦ | Quantitative |
| 45 | h-Index | (Hirsch, 2005) | Index Value ŦŦŦ | Quantitative |
| 46 | Contemporary h-Index | (Sidiropoulos, Katsaros, & Manolopoulos, 2007) | Index Value ŦŦŦ | Quantitative |
| 47 | Individual h-Index | (Harzing, 2010) | Index Value ŦŦŦ | Quantitative |
| 48 | Hi-Index | (Zhai, Yan, & Zhu, 2013) | Index Value ŦŦŦ | Quantitative |
| 49 | H2-Index | (Vanclay & Bornmann, 2012) | Index Value ŦŦŦ | Quantitative |
| 50 | M-Quotient | (Hirsch, 2005) | Index Value ŦŦŦ | Quantitative |
| 51 | G-Index | (Egghe, 2006) | Index Value ŦŦŦ | Quantitative |
| 52 | Y-Index | (Fu & Ho, 2014) | Index Value ŦŦŦ | Quantitative |
| 53 | PRP-Index | (Vinkler, 2014) | Index Value ŦŦŦ | Quantitative |
| 54 | IFQ2A index | (Torres-Salinas, Moreno-Torres, Delgado-López-Cózar, & Herrera, 2011) | Index Value ŦŦŦ | Quantitative |
| 55 | DCI-Index | (Järvelin & Persson, 2008) | Index Value ŦŦŦ | Quantitative |
| 56 | R-& AR-Indices | (Jin, Liang, Rousseau, & Egghe, 2007) | Index Value ŦŦŦ | Quantitative |
| 57 | AHP Index | (Wang, Wen, & Liu, 2016) | Index Value ŦŦŦ | Quantitative |
| 58 | Altmetric | (A. E. Williams, 2017) | Altmetric Attention Score | Quantitative |
| 59 | STAR Metrics | (Largent & Lane, 2012) | Index Value | Quantitative |
| 60 | ResearchGate-Score | (Hoffmann, Lutz, & Meckel, 2016) | Index Value ŦŦŦ | Quantitative |
| 61 | Crown indicator | (Moed, De Bruin, & Van Leeuwen, 1995) | Index Value ŦŦŦ | Quantitative |
| 62 | Societal Quality Score | (Mostert, Ellenbroek, Meijer, van Ark, & Klasen, 2010) | Index Value | Quantitative |
| 63 | PlumX Metrics | (Lindsay, 2016) | Index Value ŦŦŦ | Quantitative |
| 64 | Positive reviews of creative publications and performances | (Grant, Brutscher, Kirk, Butler, & Wooding, 2010) | Yes / NoŦ | Qualitative |
| 65 | Non-academic publications in government reports | (Penfield, Baker, Scoble, & Wykes, 2014) | How many publications are done in government reports? | Quantitative |
| 66 | Non-academic citations in government reports | (Penfield et al., 2014) | How many citations are made in government reports? | Quantitative |
| 67 | Number of industrial contracts | (ARC, 2018) | How many industrial contracts are obtained? | Quantitative |
| 68 | Amount of industrial and academic funding | (ARC, 2018) | How much funding is secured? | Quantitative |
| 69 | Community awareness of research; Collaborative projects with end users | (S. Hanney et al., 2007) | Yes / NoŦ | Qualitative |
| 70 | Facilitation and participation in expert panels for research enquiries; external institution; steering committees and advisory boards | (S. Hanney et al., 2007) | Yes / NoŦŦ | Mixed |
| 71 | Use of research outcomes, discoveries or clinical trials as a best practice | (Lewison, 2003; W. M. Trochim et al., 2008; Woolf, 2008) | Yes / NoŦ | Qualitative |
| 72 | Use of research outcome in efficiency and better performance of services | (Woolf, 2008) | Yes / NoŦ | Qualitative |
| 73 | Provision of diversified and efficient intervention and treatment options for clinicians | (Dougherty & Conway, 2008) | Yes / NoŦ | Qualitative |
| 74 | Improved client care | (Heller & de Melo-Martín, 2009; Kuruvilla et al., 2006; Mankoff et al., 2004; Pang et al., 2003; Pober et al., 2001; W. Trochim et al., 2011; Weiss, 2007; Westfall et al., 2007) | Yes / NoŦ | Qualitative |
| 75 | The decrease in events of work-environment mistakes | (Donaldson, Rutledge, & Ashley, 2004) | What is the decrease rate of work-environment mistakes? | Quantitative |
| 76 | Increase in the provision of training of healthcare improvement from the healthcare providers to the support staff | (S. R. Hanney et al., 2004; Mankoff et al., 2004; Pober et al., 2001; Sung et al., 2003) | How many support staff are trained? | Quantitative |
| 77 | Improvement in technologies and information systems for social applications | (B. Haynes & A. Haines, 1998; Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 78 | Increase in training development for system improvement | (S. R. Hanney et al., 2004; Kuruvilla et al., 2006; Lewison, 2003; Mankoff et al., 2004; Pober et al., 2001; Sung et al., 2003) | How many trainings are developed for healthcare improvements? | Quantitative |
| 79 | Creation of prevention methods for clinical practice | (Heller & de Melo-Martín, 2009; Kuruvilla et al., 2006; Mankoff et al., 2004; Pang et al., 2003; Pober et al., 2001; W. Trochim et al., 2011; Weiss, 2007; Westfall et al., 2007) | Yes / NoŦ | Qualitative |
| 80 | Adapting evidence-based practices | (Donaldson et al., 2004; Dougherty & Conway, 2008; Grant, Cottrell, Cluzeau, & Fawcett, 2000; Kuruvilla et al., 2006; Westfall et al., 2007) | Yes / NoŦ | Qualitative |
| 81 | Improvement in patient outcomes | (Donaldson et al., 2004; Dougherty & Conway, 2008; Lewison, 2003; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 82 | Improvement in health behaviours enthusiasm of patients and general masses | (Kuruvilla et al., 2006; Lewison, 2003; Woolf, 2008) | Yes / NoŦ | Qualitative |
| 83 | Development and promulgation of guidelines and policies | (Dougherty & Conway, 2008; Grant et al., 2000; S. R. Hanney et al., 2004; Brian Haynes & Andrew Haines, 1998; Kuruvilla et al., 2006; Lewison, 2003; Pang et al., 2003; W. Trochim et al., 2011) | Yes / NoŦ | Qualitative |
| 84 | Progress in personal circumstances-based healthcare e.g. based on genetic sequencing | (Mankoff et al., 2004; Zerhouni, 2007) | Yes / NoŦ | Qualitative |
| 85 | Strengthening of service-client relationship | (Woolf, 2008) | Yes / NoŦ | Qualitative |
| 86 | Research outcome translation into medical practice for improvement | (Dougherty & Conway, 2008; Kessler & Glasgow, 2011) | Yes / NoŦ | Qualitative |
| 87 | Strengthening human protection through improved policies and better procedures | (Weiss, 2007) | Yes / NoŦ | Qualitative |
| 88 | Improvement in regulation for introducing advanced technologies, tools and techniques | (Lewison, 2003) | Yes / NoŦ | Qualitative |
| 89 | Compliance of ethical guidelines in research | (Kuruvilla et al., 2006; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 90 | Development of community-based awareness | (Sarli et al., 2010) | Yes / NoŦ | Qualitative |
| 91 | Betterment of policies, guidelines and reimbursement systems for service providers | (Sarli et al., 2010) | Yes / NoŦ | Qualitative |
| 92 | Increased empowerment of service users | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 93 | Support of research outcome and information for political decision and policy-making | (Buxton & Hanney, 1996; B. Haynes & A. Haines, 1998; Kalucy et al., 2009; Pang et al., 2003) | Yes / NoŦ | Qualitative |
| 94 | Improved public awareness about the environment and culture, Public behaviour change and advocacy; Increased literacy and numeracy rates | (Grant et al., 2010; Raftery et al., 2016) | Yes / NoŦ | Qualitative |
| 95 | Improvement in health literacy of health users and patients | (Kuruvilla et al., 2006; Pang et al., 2003) | Yes / NoŦ | Qualitative |
| 96 | Improvement in health status of health users and patients | (Dougherty & Conway, 2008; Kuruvilla et al., 2006; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 97 | Establishment of public health, education or any other social schemes for a region | (Woolf, 2008) | Yes / NoŦ | Qualitative |
| 98 | The decrease in social disparities | (Heller & de Melo-Martín, 2009; Kuruvilla et al., 2006; Zerhouni, 2007) | Yes / NoŦ | Qualitative |
| 99 | Improvement in inter-organizational coordination for betterment in social sector | (Sarli et al., 2010) | Yes / NoŦ | Qualitative |
| 100 | Increase in planning efforts and program implementation related to social issues | (Heller & de Melo-Martín, 2009; Woolf, 2008) | Yes / NoŦ | Qualitative |
| 101 | Improvement in health user about health research | (Weiss, 2007) | Yes / NoŦ | Qualitative |
| 102 | Increased empowerment and knowledge of health users about health issues | (Kuruvilla et al., 2006; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 103 | Better communication and perception of health users about health risks | (Kuruvilla et al., 2006; Pober et al., 2001; Weiss, 2007) | Yes / NoŦ | Qualitative |
| 104 | Expansion of health education, literacy and other social advantages | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 105 | Improvement in Occupational Health and Safety Environment | (Raftery et al., 2016; V. Williams, Eiseman, Landree, & Adamson, 2009) | Yes / NoŦ | Qualitative |
| 106 | Disuse the law for obsoleting the existing method of drug approval | (Maliha, 2018) | Yes / NoŦ | Qualitative |
| 107 | Commercialization of new discovery, product or technology | (Kuruvilla et al., 2006; Lavis et al., 2003; Woolf, 2008) | Yes / NoŦ | Qualitative |
| 108 | Improvement in cost reducing techniques and effectiveness | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 109 | Improvement in economic gains such as increased employment, health cost cut | (Aries & Sclar, 1998; S. R. Hanney et al., 2004; Kalucy et al., 2009; Kuruvilla et al., 2006; RAND Europe, 2006; Weiss, 2007) | Yes / NoŦŦ | Mixed |
| 110 | Development of new job opportunities and growth in the specific economic sector or geographical region | (Aries & Sclar, 1998) | Yes / NoŦŦ | Mixed |
| 111 | Development of medicinal products and therapeutic procedures | (S. Hanney et al., 2007; Sarli et al., 2010) | How many products or procedures are developed? | Quantitative |
| 112 | Improvement in a business environment, commercialization, technology incubation, products and processes | (Buxton & Hanney, 1996) | Yes / NoŦ | Qualitative |
| 113 | Reduction in work loss due to illness and increased benefits from a healthy workforce | (CAHS, 2009) | Yes / NoŦ | Qualitative |
| 114 | Increased Royalties, employment, Licences; creative works commissioned | (Grant et al., 2010) | Yes / NoŦŦ | Mixed |
| 115 | Creation of new knowledge about sustainable development and environmental protection for better future of the world | (Kuruvilla et al., 2006) | Yes / NoŦ | Qualitative |
| 116 | Improved environmental quality and sustainability | (Engel-Cox, Van Houten, Phelps, & Rose, 2008) | Yes / NoŦ | Qualitative |
| 117 | Reduced emissions; regeneration or arrested degradation of natural resources | (Raftery et al., 2016) | Yes / NoŦŦ | Mixed |
| 118 | Improved awareness of environmental impacts and legislation for protection | (CAHS, 2009) | Yes / NoŦ | Qualitative |
| 119 | development of mitigation methods for reducing environmental hazards and losses from natural disasters | (Grant et al., 2010) | Yes / NoŦŦ | Mixed |
Ŧ In case of Yes, description and justification is needed. ŦŦ In case of Yes, detailed case study with quantitative evidence is needed. ŦŦŦ Bibliometric indicator. |
References
ARC. (2018). Excellence in Research for Australia (ERA) 2018: Submission Guidelines. Retrieved from http://www.arc.gov.au/sites/default/files/filedepot/Public/ERA/ERA%202018/ERA% 202018%20Submission%20Guidelines.pdf
Aries, N.R., & Sclar, E.D. (1998). The economic impact of biomedical research: a case study of voluntary institutions in the New York metropolitan region. J Health Polit Policy Law, 23(1), 175-193. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/9522285
Buxton, M., & Hanney, S. (1996). How can payback from health services research be assessed? J Health Serv Res Policy, 1(1), 35-43.
CAHS. (2009). Making an Impact: A Preferred Framework and Indicators to Measure Returns on Investment in Health Research. Retrieved from Otawwa, Canada:
Dougherty, D., & Conway, P.H. (2008). The “3T’s” road map to transform US health care: the “how” of high-quality care. Jama, 299(19), 2319-2321. Retrieved from https://jamanetwork.com/journals/jama/articlepdf/181916/jco80037_2319_2321.pdf
Garfield, E. (2006). Citation indexes for science. A new dimension in documentation through association of ideas. 1955. Int J Epidemiol, 35(5), 1123-1127; discussion 1127-1128. doi:10.1093/ije/dyl189
Gordon, M., & Meadows, A. (1981). The dissemination of findings of DHSS funded research. Primary Communications Research Centre, Leicester: University of Leicester.
Grant, J., Brutscher, P.-B., Kirk, S.E., Butler, L., & Wooding, S. (2010). Capturing Research Impacts: A Review of International Practice. Documented Briefing. Rand Corporation.
Grant, J., Cottrell, R., Cluzeau, F., & Fawcett, G. (2000). Evaluating “payback” on biomedical research from papers cited in clinical guidelines: applied bibliometric study. Bmj, 320(7242), 1107-1111. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC27352/pdf/ 1107.pdf
Hanney, S., Buxton, M., Green, C., Coulson, D., & Raftery, J. (2007). An assessment of the impact of the NHS Health Technology Assessment Programme. Health Technol Assess, 11(53), iii-iv, ix-xi, 1-180.
Hanney, S.R., Grant, J., Wooding, S., & Buxton, M.J. (2004). Proposed methods for reviewing the outcomes of health research: the impact of funding by the UK’s’ Arthritis Research Campaign’. Health Research Policy and Systems, 2(1), 4. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC503400/pdf/1478-4505-2-4.pdf
Harzing, A.-W.K. (2010). The publish or perish book: Tarma software research Melbourne.
Haynes, B., & Haines, A. (1998). Barriers and bridges to evidence based clinical practice. Bmj, 317(7153), 273-276. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/9677226
Haynes, B., & Haines, A. (1998). Barriers and bridges to evidence based clinical practice. Bmj, 317(7153), 273-276. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 1113594/pdf/273.pdf
Heller, C., & de Melo-Martín, I. (2009). Clinical and Translational Science Awards: can they increase the efficiency and speed of clinical and translational research? Academic Medicine, 84(4), 424-432.
Kalucy, E.C., Jackson-Bowers, E., McIntyre, E., & Reed, R. (2009). The feasibility of determining the impact of primary health care research projects using the Payback Framework. Health Research Policy and Systems, 7(1), 11.
Lewison, G. (2003). Beyond outputs: new measures of biomedical research impact. Paper presented at the Aslib Proceedings.
Lindsay, J.M. (2016). PlumX from plum analytics: not just altmetrics. Journal of Electronic Resources in Medical Libraries, 13(1), 8-17.
Maliha, G. (2018). Obsolete to Useful to Obsolete Once Again: A History of Section 507 of the Food, Drug, and Cosmetic Act.
Moed, H., De Bruin, R., & Van Leeuwen, T. (1995). New bibliometric tools for the assessment of national research performance: Database description, overview of indicators and first applications. Scientometrics, 33(3), 381-422.
Nathan, D.G. (2002). Careers in translational clinical research—historical perspectives, future challenges. Jama, 287(18), 2424-2427. Retrieved from https://jamanetwork.com/journals/jama/articlepdf/194890/JCO20035.pdf
Pang, T., Sadana, R., Hanney, S., Bhutta, Z.A., Hyder, A.A., & Simon, J. (2003). Knowledge for better health: a conceptual framework and foundation for health research systems. Bull World Health Organ, 81(11), 815-820. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/ 14758408
RAND Europe. (2006). Measuring the benefits from research. Cambridge, England. Retrieved from https://www.rand.org/content/dam/rand/pubs/research_briefs/2007/RAND_RB9202.pdf
Sung, N.S., Crowley, W.F., Jr., Genel, M., Salber, P., Sandy, L., Sherwood, L.M., ... Rimoin, D. (2003). Central challenges facing the national clinical research enterprise. Jama, 289(10), 1278-1287. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/12633190
Westfall, J.M., Mold, J., & Fagnan, L. (2007). Practice-based research—“Blue Highways” on the NIH roadmap. Jama, 297(4), 403-406. Retrieved from https://jamanetwork.com/journals/jama/articlepdf/205216/jco60049_403_406.pdf
Williams, V., Eiseman, E., Landree, E., & Adamson, D. (2009). Demonstrating and Communicating Research Impact. Preparing NIOSH Programs for External Review. Retrieved from