Hospitals affiliated with universities are relevant elements of academic systems where education and research take place (
Washington et al., 2013). Nevertheless, there are significant differences in the types of relationships between hospitals and universities both on an international and national level: on one end of the spectrum there are fully integrated hospitals and medical faculties, while on the other end there are non-integrated hospitals offering clinical placements for students. In between lies an array of structures at varying degrees of interdependency, all determined by national and regional systems.
Examining the organizational structures of university-affiliated hospitals, Wartman describes two prototypical models of academic health centres, while Levine considers five possible structures with varying degrees of interdependency (
Levine, 2002;
Wartman, 2015). For the purpose of the Leiden Ranking, we identify three general models for relationships between universities and hospitals:
1. full integration of the hospital and the medical faculty into a single organization;
2. health science centres in which hospitals and medical faculty are still separate entities, albeit within the same governance structure;
3. structures in which universities and hospitals are separate entities and collaborate with one another.
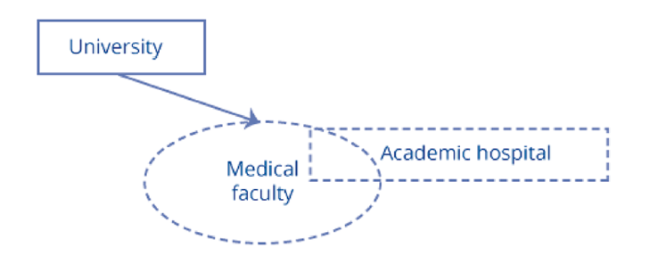
The case of fully integrated academic hospitals shows a strong degree of interdependency with a particular university, for example, when the medical faculty is located at the hospital or vice versa (see Figure 1). This model is found in most academic hospitals of Belgium, the Netherlands, Germany, and Switzerland.
Figure 1. Full integration model. |
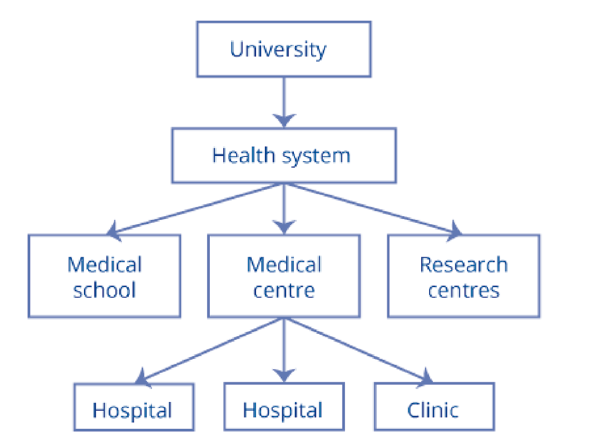
The system of Health Science Centers also presents a strong degree of interdependency between academic hospitals and universities but the structure differs from the full integration model. In the full-integration model, the medical faculty and hospital are often the same institution. Health science centres, on the other hand, are organizations that coordinate the medical faculty, the various patient-oriented medical facilities, and the research centres (see Figure 2). They can fall directly under the university or stand as a separate legal entity. Health science centres exist predominantly in the United States of America (e.g. the UNM Health Sciences Center in New Mexico).
Figure 2. Health science centres. |
It is important to note the difference between health science centres (as modelled in
Figure 2) and academic health science networks such as the
Oxford Academic Health Science Network in the United Kingdom. These health networks refer to partnerships between one or more universities, local governments, and industries that seek to improve innovation delivery times and patient services (
Fish, 2013). We have found that health networks are rarely mentioned in publications; furthermore, we have found that they pursue varied interests and do not focus primarily on undergraduate education. Other networks such as the
Copenhagen University Hospital in Denmark and the
University Health Network in Canada refer to collaboration agreements between the regional health authorities and a university without institutionalized integration between the medical faculty and all the hospitals in said regions.
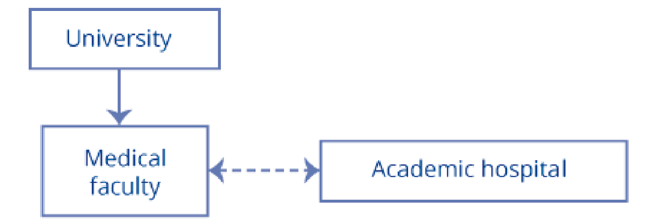
The third model refers to a relationship of collaboration and support between hospital and university in which the collaboration is structural rather than incidental: there are some shared activities between the two, but no full integration of the medical faculty into the hospital (see Figure 3). These types of relationships are the most common worldwide.
Figure 3. Collaboration and support. |
Around the world, hospitals are referred to as “academic hospital”, “teaching hospital”, “university hospital”, “third-tier hospital”, and “academic medical centre” to denote some form of collaboration with a university; however, these nomenclatures do not constitute universally accepted definitions of specific types of hospital-university relationship, and thus can denote different things in different countries or even regions of the same country (
Shi et al., 2021;
Sato & Fushimi, 2012). Additionally, the level of collaboration between a university and a hospital may vary substantially between countries and regions, further rendering such labels unsuitable for global comparisons.
Sometimes the relationship between a hospital and a university may seem clear according to local perceptions. However, such local understandings of the interconnectedness between hospitals and universities cannot be used for international comparisons as they are not sufficiently consistent and demand specific local knowledge. On a similar note, some bibliometric databases assign affiliation between teaching/academic hospitals and universities based on local perceptions as communicated by each university to the database owner. This approach presents also shortcomings when doing international comparisons as it lacks consistency and depends on the client base of the various databases.
Following our previous work on academic hospitals (
Praal et al., 2013), we at the Leiden Ranking have developed a three-step workflow to classify the relationship between universities and their affiliated hospitals. This workflow effectively transposes the three above-noted relationship models into the two types of instrumental relationships that the Leiden Ranking employs for the allocation of the publication output of academic hospitals. We distinguish between academic hospitals that are associated with universities (“associate”) and academic hospitals that can be considered as part of the university (“component”).
When a hospital and a medical faculty are fully integrated or when a hospital is part of a health science centre (see Figures 1 and 2) the relationship is classified as component. When a hospital follows the model of collaboration and support (see Figure 3) the relationship is classified as associate. Although distinct in their organizational structures, the full-integration and health science centre models suggest a strong integrated relationship concerning the tasks of education and research. In both cases the medical faculty is difficult to separate from the hospital; therefore we treat them in the same way. In the collaboration and support model this is not the case.
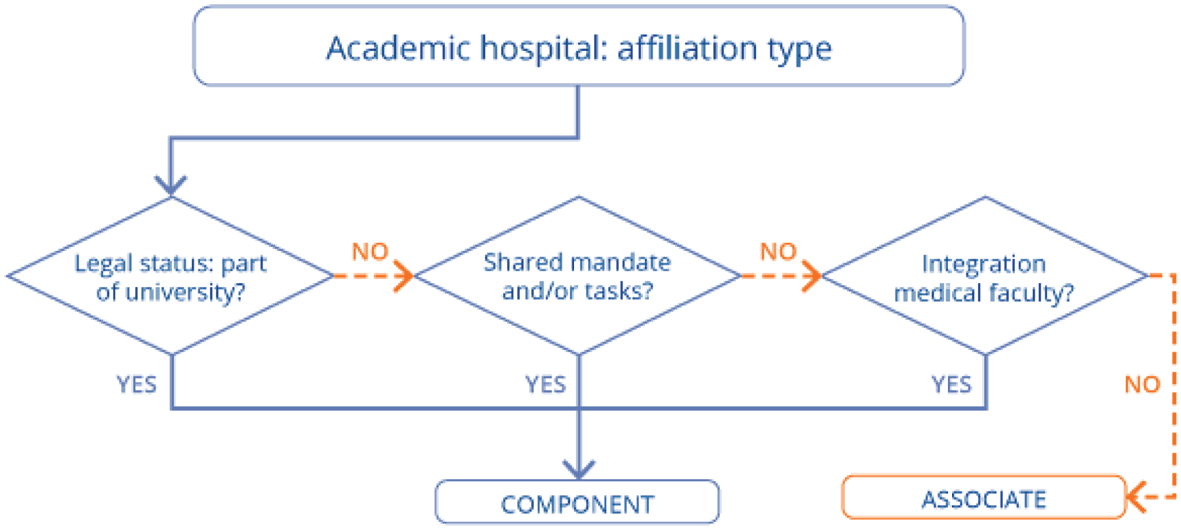
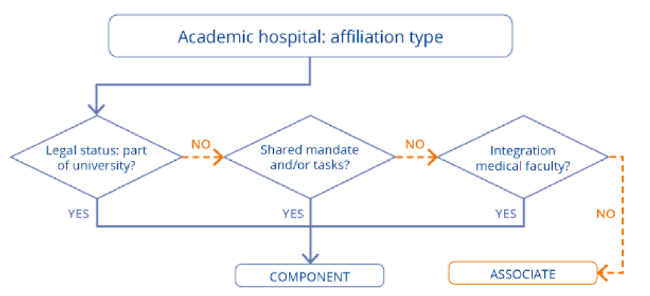
Although the proposed scheme cannot do justice to the myriad forms of integration that might exist, it seeks to address the complexity of the relationship between academic hospitals and universities. The scheme is pragmatic and focuses on three aspects that can aid in evaluating the degree of interdependence: legal status, shared educational mandate, and level of physical integration (see Figure 4).
Figure 4. Three-step workflow. |
First, a hospital's legal status is examined. If the ownership lies with the university or a foundation owned by or related to the university, the hospital is considered a component. In many cases, ownership can be easily determined for a whole country or region given specific health services regimes. For example, in the United Kingdom, hospitals and trusts that collaborate intensively with universities are owned by the National Health Service. In Poland, hospitals strongly connected to universities became part of the university structure by law in 2001. Thus according to this first step, hospitals in the United Kingdom cannot be considered as components, while academic hospitals in Poland should be considered as components of their universities.
For the first step in the workflow, not only the direct legal ownership is considered but also whether the hospital is part of a university health system. We find many cases like this in the United States of America. For example, the Duke University Health System comprises three hospitals, a medical faculty, and a series of outpatients' clinics. Northwestern Medicine has a similar structure that comprises various hospitals, a medical school, and a comprehensive cancer centre. Notably, an organizational structure like that of Duke or Northwestern is significantly different from a health science network as mentioned above, where the affiliated university exercises no direct control over the management of hospitals, clinics, and medical faculties.
Some cases present a seemingly opposite ownership situation that nevertheless results in a classification as component. For example, the Mount Sinai Health System in the United States of America owns the Icahn School of Medicine. This medical school was previously considered as part of City University of New York (1968-1998) and New York University (1999-2007) because these universities were granting its degrees until 2010; since then, Mount Sinai has been accredited as an independent degree-granting institution. Technically, the medical school belongs to the hospital group, yet for the Leiden Ranking's practical purposes (publication count) the hospital group is seen as a component of the medical school.
The second step in the workflow examines a hospital's mandate. Given the Leiden Ranking's focus on universities, the tasks considered here are core-curriculum education and research. In general, every hospital affiliated with a university will conduct research, except for smaller clinics which solely provide clinical placements. A more difficult function to determine is the type of education provided by a hospital. Over all, we have found that hospitals provide different levels of education ranging from patient education (for example on nutrition), specialist training or continuous education, to core-curriculum education for undergraduate students. On some occasions, a hospital has a clear mandate to aid a university in the provision of undergraduate education, in which case the hospital is considered to act as a component of the university.
The mandate of a hospital is not always publicly available, although for some countries it is part of the national or regional legislation. In a few cases, the mandate is part of a hospital's mission statement. For example, the Centre hospitalier universitaire de Poitiers in France mentions two types of education under its mission. The first type is referred to as “prevention and education”, and targets patients as well as professionals. The second type concerns education for students of the University of Poitiers' medical faculty, including undergraduate education. In this case, although there is no mention of an explicit mandate, the hospital's mission does seem to indicate that it should be considered as a component. In instances like this wherein the mandate is not sufficiently clear, a full assessment following the three-step workflow is necessary in order to definitively determine whether the university-hospital relationship is associate or component.
In some countries, we have observed a clear pattern in which public academic hospitals provide core education. However, it is possible that the wave of public-services privatization in those countries may influence the extent of educational tasks provided by hospitals, as privatized hospitals tend to become less involved with education. In Germany, for example, the majority of large academic hospitals are traditionally public and involved with core education, but as some of these hospitals have been recently privatized, not all German hospitals can be automatically considered as components of universities.
Often, information about hospitals' mandates is not available at all. For example, the Turku University Hospital is owned by the Hospital District of Southwest Finland and seems to only cover continuous education for specialists. For such cases, which are the majority, the assessment requires progressing to the next step of the workflow.
The third and final step of the workflow examines to what extent a hospital and medical faculty are integrated. This step covers two major elements: the physical location of the faculty and the publication behaviour of authors mentioning the hospital affiliation. For the former we consider whether the hospital and the medical faculty have shared locations. For the latter we examine whether the authors publishing for the hospital are members of the medical faculty.
When a hospital shares locations and staff with a medical faculty, it is considered a component of the university. As in the previous steps, the outcome of this review is rarely a binary yes-no. In some cases, the medical school or most of its departments will be located on the hospital grounds, indicating a tight physical integration. For example, the medical school of University of Bari Aldo Moro in Italy is located at the Azienda Universitaria Ospedaliera Consorziale - Policlinico Bari. Yet what we often find is that only one or two departments out of many are located at the hospital: usually pediatrics, gynaecology, clinical medicine, or nursing. Such is the case of Hospital Clínico San Carlos which houses the gynecology and obstetrics departments of the Complutense Universityin Spain. In those cases, we do not consider this as a tight physical integration.
With this complexity in mind, the third step also considers the publication behaviour of authors using the hospital affiliation: we examine a sample of publications comprising authors using the hospital affiliation without mentioning the university to which the hospital is supposedly affiliated. We then investigate whether those authors are formally employed by the university. For example, the majority of the authors from our sample who publish using the Canberra Hospital affiliation are employed by the Australian National University. It is a sign of strong interdependency when the majority of authors publishing for a hospital are also faculty members at its affiliated university.
2.2.4 Evaluating the three steps
When the workflow shows a low level of interdependency, we classify the relationship of the hospitals as that of associate to the university. As an example, a hospital owned by the regional health authority, without a clear mandate for core-curriculum education, with one or no university department located on the hospital premises, and few authors publishing with the hospital's address who hold a faculty position, would be considered as associate. Such is the case of the Institutul Clinic Fundeni to the Carol Davila University of Medicine and Pharmacy of Bucharest.
It is worth emphasizing that this is not a straightforward process: often it is difficult or impossible to retrieve all the information necessary to complete the workflow, and even with all of the information, the results of the assessment may be ambiguous. Thus the decision of classifying the relationship as associate or component typically depends on a combination of the available information. Lastly, because of its resource-intensive nature, the assessment is only carried out for academic hospitals whose publication output surpasses a specific threshold.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}